
Leveraging Digital Health Master Plan for COVID-19

For governments to effectively manage the health crisis caused by COVID-19, they must have the ability to make decisions based on reliable and consolidated data.
Today, the data that are key in this decision making are those related to the availability and location of health facilities.This is specifically true in low- and middle-income countries. Identifying the infrastructure facilities will allow governments to allocate the necessary funding to the essential health services.
During a crisis, time is critical. Governments must be able to rely on what has already been accomplished to improve the information system and health surveillance. Those who started this work before the crisis will have a head start. They will already have critical data at their disposal to manage the crisis. This kind of data management and collection should not stop during the crisis. On the contrary, it is one of the crucial elements of health risk management and mitigation.
In the below, based on Bluesquare experience in the DRC and Niger, we describe the approach to leverage Digital Health Master Plan to tackle COVID-19.
Initial and ongoing work to build the Digital Health Master Plan
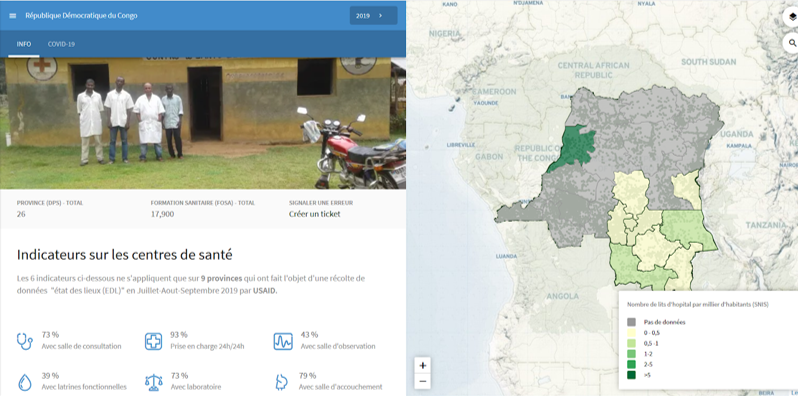
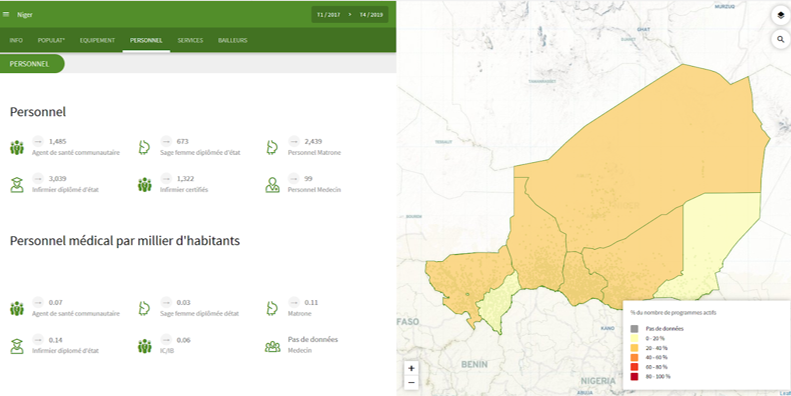
We have been supporting the DRC and the Niger Ministries of Health in the implementation of an interactive and dynamic health map of public and private health facilities (pharmacies, clinics and health centres).
The results of this work provide routine information. It takes into account the health pyramid and population, to the health authorities (the Minister, Technical and Regional Directorates of the Ministry, Health Districts, Projects and Programmes, Partners, external agencies, NGOs, hospitals and health workers). With this information, they can better allocate resources and target underserved regions and populations.
Bluesquare has specifically focused on identifying databases containing GPS coordinates of health structures. They provide precise information, such as photos and features that are specific to the DRC and Niger. In Niger, we identified 14 different databases, including the one from the SNIS (HMIS).
We also identified new sources of data to help increase the number of GPS coordinates on the health map, based on existing data. In the DRC, we have identified the following databases: Geolocation of health facilities in the Ebola response, a database from MSF/common geographical repository, a database from the PDSS containing the GPS coordinates of about 500 health facilities in Kinshasa and Kasai.
These multiple data sources, combined with a constant change of data (population estimates from remote sensing, settlement location, names of villages and settlements, health areas, health districts, health facilities and “découpage communal”), inconsistency between sources (for example, the health layer does not always correspond to the administrative layer) require continuous integration.
Thanks to our visualisation tool, Dataviz, we have set up public portals to visualise the ongoing work on the health map (carte sanitaire) in Niger and the DRC.
Work that facilitates a quick response to COVID-19
In the framework of the COVID-19 response, countries must quickly identify the infrastructures and services they have to address the disease and to target funds to acquire the ones still needed.
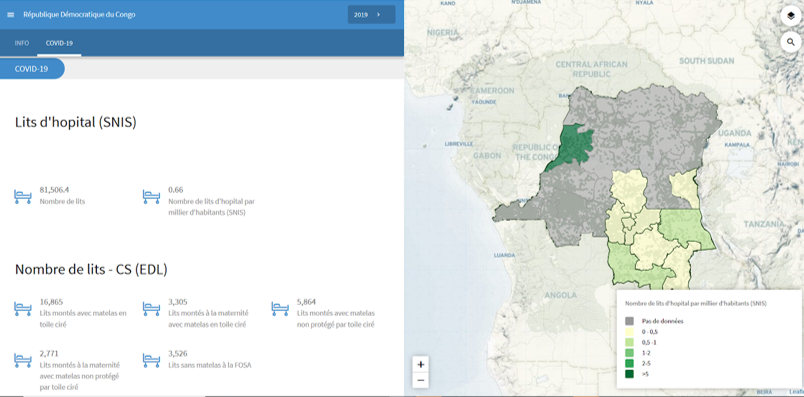
In the DRC, we have been working with the Health Ministry to support health information systems and help the government create a health map. We are currently working with the national COVID-19 Task Force to help them tackle the disease.
We are providing support for the geolocalisation of the COVID capacity response. This includes screening devices, in-patient beds, ventilator beds, critical care beds, laboratories, oxygen production units, etc..
The work that has been done, and which is continuing with the health map (“carte sanitaire”), supports the establishment of an “état des lieux” of the existing infrastructures and services for a COVID response. We are putting in place an android app for the “carte sanitaire” update.
We are also investigating other databases that provide integrated information on the COVID Capacity response. The aim is to consolidate data into a single digital database.
This work, while seemingly low-impact, reveals its importance with the COVID-19 pandemic. Ministries of Health and different stakeholders are even more tempted to work with non-centralised databases. They gather data through excel files and share them by email, creating different versions of the same database. More than ever, a centralised digital database, to which the different actors can contribute, is critical.
In the first phase, Bluesquare partnered with the Agence Nationale d’Ingénierie Clinique d’Information et d’Informatique de Santé or ANICiiS. Together, we are identifying the different existing data flows and databases to have a clear view of the full process (what kind of data exist, how data are gathered, by who, and how often etc..). We invited the different partners to share any complementary existing databases. When complete, the second phase is to propose a set of tools that take into consideration the actual flow of information, while switching from a decentralised multi-source database to one central tool.
This information will be made publicly available via the public data visualisation interface: “STOP COVID“
Get more information about Bluesquare’s support to COVID-19 response.



